

A 64yr old lady comes to see you, complaining of breathlessness on minimal exertion over the past 6months. She denies any chest tightness or discomfort.
She has no past cardiac history, and has always enjoyed a healthy lifestyle.
She takes no medication.
Examination in unremarkable. She appears slim and healthy, is normotensive, with a regular pulse rate of 80 bpm, and no murmurs.
You arrange some routine bloods, which are normal, and an ECG. Her serum BNP comes back at 38.
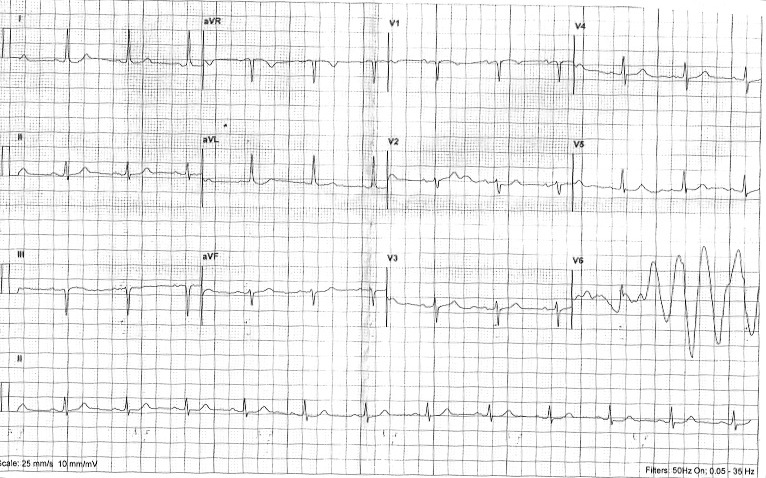
Her ECG is below. The digital ECG machine interpretation reports :
Sinus rhythm
Multifocal ventricular extrasystoles
Run of ventricular extrasystole
Inferior myocardial infarct, age undetermined.
What do you think?
Lets take each of these statements in turn.
Q1. Is this sinus rhythm? (Can you see P waves, and if so are they regular and associated with every QRS?)
Yes. We’re happy with the machine’s analysis that this is Sinus rhythm, because for every P wave there is a QRS complex.
Q2. Can you see the multifocal ventricular extrasystoles, or the run of ventricular extrasystoles?
As far as the first statement goes, there are no isolated dysmorphic beats that resemble a ventricular ectopic. As for the “Run of ventricular extrasystoles” – this is of course, it’s referring to lead V6. But what about this?
Remember, that each ‘column’ on an ECG trace, records the heart rate at the same moment in time for all 3 leads in that column. So the first column simultaneously records the view from the limb leads (I, II and II). The recording will then switch to the second column, which in turn records simultaneous beats in the Augmented limb leads (AvR, aVL, avF). The third column records V1, V2 and V3 simultaneously, and the fourth records V4,V5 and V6.
Whilst the heart rate and rhythm might well change between columns, within each of the columns it should always remain the same.
So, how could a run of VE’s appear in V6 but not in V4 and V5?
It couldn’t!
The only explanation for the anomaly in V6 is artefact. Mostly likely the V6 badge was knocked, or lost contact. We are not concerned about this pattern at all!
Q3. Is this ECG consistent with an Inferior MI?
Aha. We have now reached the real point of this ECGclass.
How often do we see a computer generated report “Inferior infarct cannot be ruled out” or “possible anterior infarct, aged undetermined”.
This is a very common reason for otherwise well patients, or those with clearly non-cardiac chest pain, to be referred for a cardiology opinion. This can cause unnecessary alarm for the patient.
In short, no, this ECG is not suggestive of an old MI.
In this lady, once I’d ruled out possible angina (by taking a more detailed history), I’d be looking for other, non-cardiac, causes of her breathlessness.
So lets talk about Q waves…..
Pathological Q waves – or not?
When are the Q waves pathological?
A pathological Q wave is a result of absence of electrical activity, following myocardial damage. They generally take several hours to develop after an MI, and usually persist indefinitely.
The exception to this is if seen during an acute MI, but the myocardial tissue is reperfused early by Primary PCI (Percutaneous Coronary Intervention). The myocardial tissue can then recover, and the pathological Q waves disappear.
To be pathological there are a couple of simple rules of thumb:
- The depth of the Q wave should be at least 25% of the depth of the associated R wave
- The pathologically deep Q wave should appear in at least 2 contiguous leads (An isolated Q wave to lead III is a very common normal variant)
- Any Q wave in leads V1- V3 with a duration of >0.02seconds is likely to be pathological.
- Many ‘apparently’ pathological Q-waves, often infact have a tiny R-deflection preceeding them – this can be so small it may need searching closely for. (seen in example 1 above).
- A pathological Q wave may also be broad, in appearance, but again, must be seen in two contiguous leads.
There are many more detailed criteria suggested for Pathological Q waves, if you are interested, search for either the ESC classification; the Minnesota Code Classification System; or the Novacode system.