

A new ECG is launched most Monday and Wednesday evenings.
Cases are generally aimed at healthcare students and professionals.
All scenarios are completely fictitious and theoretical, but based on commonly occurring presentations in practice.
This is an educational site, intended for healthcare professionals and shouldn’t be construed as patient advice.
Remember to use the #pulsemdx
An 82yr old lady is brought to see you by her daughter.
She is complaining of intermittent dizzy spells.
On examination, the lady appears frail, but clinically well. Her BP is good and heart sounds are normal. Her pulse seems a bit irregular, but not fast.
See the ECG below:
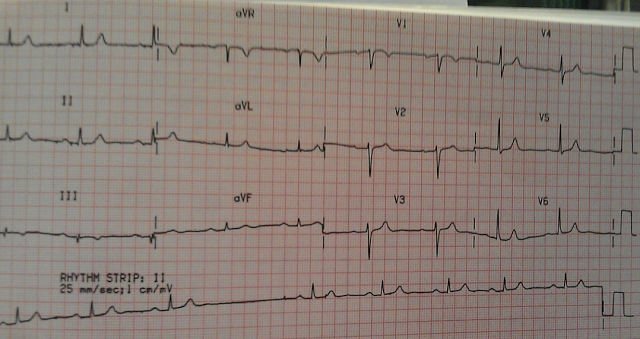
The ECG shows a Sinus bradycardia, with a variable rate of around 50 beats per minute. (Remember how to calculate the rate of an irregular ECG? Count the number of complexes in 6 seconds and multiple this by 10. Assuming paper speed of 25mm/sec then 6 seconds = 30 large squares). Now study the Lead II rhythm strip. There are P waves in front of every QRS complex, and the P waves appear morphologically constant and normal; as do the QRS complexes. Every P wave is conducted. The PR interval is constant, but slightly prolonged (at just over the max. of 5 small squares, or 0.20 secs). So a First degree AV block is present. But that’s not all.
You also note a ‘pause’ on the long lead II. No P wave (and no QRS complex) occurs when expected. If this pause was interrupted by an odd looking QRS complex, this would be called an “escape” beat originating from an abnormal site within the ventricular wall. However, no escape beats are seen, and the pause is terminated by a sinus beat. You are concerned about the ECG and ask a bit more about her dizzy spells.
Her daughter is discloses that she is worried, that on at least one occasion, she thinks her mother may have transiently ‘blacked’ out.
Q2. What are you thinking now?
You decide to get a long lead II rhythm strip to help you: 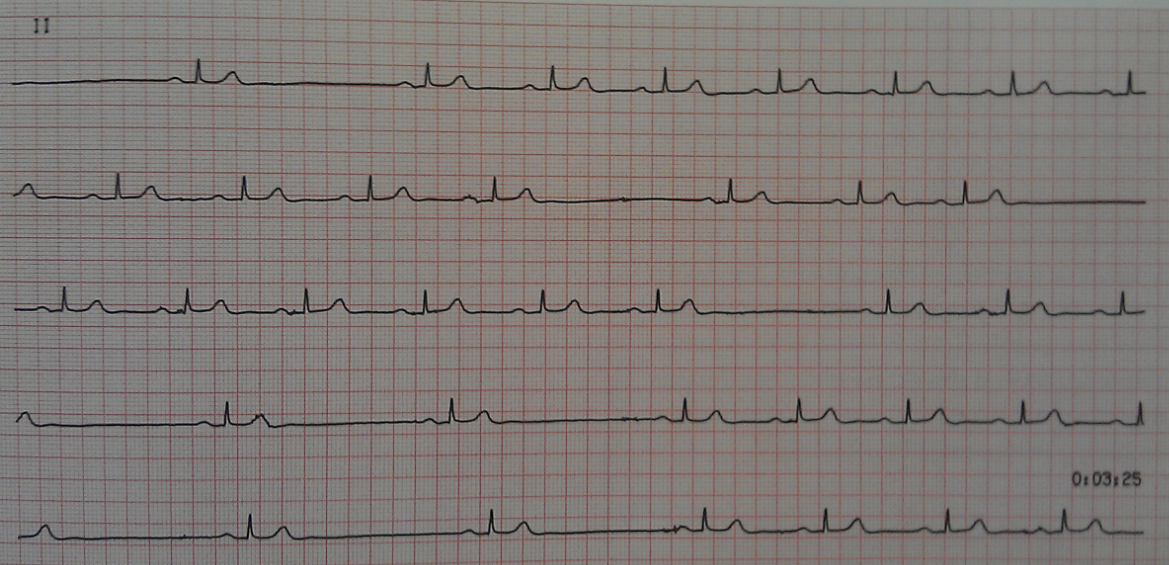 What do you think of the pauses now?
What do you think of the pauses now?
This looks a bit more sinister. Far more pauses can be seen. The duration of each pause is double the basic R-R interval. The ECG’s show Sino-Atrial block. You may want to do ambulatory ECG recording to look for longer pauses (ie. failed conduction of several consecutive sinus beats, which will gives pause durations in multiples of the basic R-R interval). Given this lady’s symptoms of possible blackouts, she probably needs admitting, or urgent referral, for permanent pacing. Sino-atrial block is one form of Sino-Atrial Dysfunction, or Sick Sinus syndrome.
Others types include Sinus Pause, Sinus arrest, and Bradycardia-Tachycardia Syndrome.
SA Dysfunction is a sign of diseased tissue around the sino-atrial node. This may be damage secondary to an MI , or to a degenerative ageing process affecting the node. Although the sinus node depolarises normally, there is intermittent failure of that impulse being conducted through the atrial tissue.
Summary
The ECG above shows:
1. A Sinus Bradycardia
2. A First degree A-V block
3. A Sino-Atrial Block
Lessons:
1. Be very suspicious if you ever suspect Sinus Arrhythmia in the elderly. Sinus arrhythmia occurs with respiration in the young and healthy. The rise and fall of the heart rate is gradual with respiration. In the elderly, sinus arrhythmia is rare. Study the R-R interval, if the distance is always in multiples of the basic rate, then a Sino-Atrial block is far more likely in this age group.
2. Look very carefully for P-waves:
Atrioventricular (AV)Heart Blocks
A First degree AV heart block (prolonged PR interval) results when each wave is conducted from the Sino-Atrial node to the ventricles, but something slows it down.
A Second degree AV heart block would be present if all the P waves are normally conducted, but occasionally a wave is not conducted to the ventricles at the Atrio-ventrcular node; nor through the Bundle of His. (i.e. Not all P-waves are followed by a QRS).
There are 3 variations of second degree Heart Block:
- Mobitz Type I or Wenckebach (Usually benign)
- Mobitz Type II (may trigger a complete heart block)
- 2:1 or 3:1 Conduction type (May trigger a complete heart block)
A Third degree AV heart block
Atrial contraction is normal, but no beats are conducted to the ventricles. To compensate, the ventricles are excited by a “slow escape” mechanism, starting from an abnormal focus within the ventricles. Thus the atrial rate is normal, but the ventricular rate is often very slow.
There is no relationship between the P waves and the QRS waves.
Sino-Atrial (SA) Heart Blocks
A Sinus Block occurs when there is complete failure of the sinus node to depolarise the atrium.
In a sino-atrial block, the P-P interval remains regular (as in above ECG) but an entire PQRS complex will be occasionally missing.
Thank you for your time.