

Lesson 13
Cases are generally aimed at healthcare students and professionals.
All scenarios are completely fictitious and theoretical, but based on commonly occurring presentations in practice.
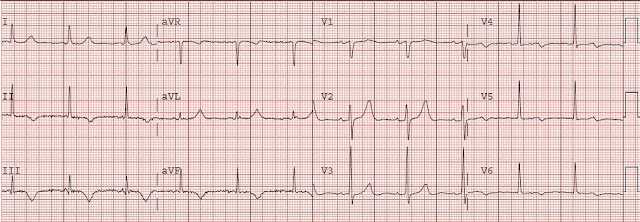
A 22-year-old male presents with agitation and delirium after smoking an unknown substance that an equally unknown person on the street offered him. You note a rapid radial pulse at around 150 bpm and attach him to the cardiac monitor:

Well now we’re in a tough spot. It’s difficult to tell whether the ECG shows sinus tachycardia or some non-sinus narrow-complex tachycardia (we’ll use the colloquial shorthand of “SVT” to include all those other options on the differential, including AVNRT, AVRT, ectopic atrial tachycardia, junctional tachycardia, etc…). If it is indeed sinus tach, then the requisite P-waves must be those upright deflections in II and III and superimposed on the T-waves.
Is there something we could do to see if those really are P-waves buried in the T-waves?